hourlong learnings #3: how TENS talks to nerves and why therapeutic dose is key
A TENS unit is a battery, waveform generator, current-control circuit, and a few electrodes. It sends pulsed current through the skin to recruit nearby nerve fibers. The goal is not to repair a strained muscle, realign a joint, or remove inflammation. It is to change the neural traffic associated w/ pain.
A rough model is:
$$ \text{waveform} \rightarrow \text{electric field in tissue} \rightarrow \text{axon recruitment} \rightarrow \rightarrow \text{temporary pain relief} $$
I started using TENS after spending weeks looking for remedies for injuries around my neck, back, and shoulders. The relief was noticeable, although the device gave me almost no explanation for why one placement felt broad and useful while another felt sharp, weak, or caused a muscle twitch.
1. the CNS and PNS are the basic map
The nervous system can first be split into two large parts:
CNS:
brain and spinal cord
PNS:
cranial nerves, spinal nerves, roots, ganglia, and peripheral nerve branches
outside the brain and spinal cord
The peripheral nervous system carries information in both directions. Afferent fibers carry sensory information toward the CNS. Efferent fibers carry motor and autonomic commands away from it.
TENS is applied at the body surface, so the first excitable structures it can reach are in the PNS. The resulting action potentials then propagate along axons toward the spinal cord, where they can alter how nociceptive input is processed.
The pathway is roughly:
$$ \text{skin/muscle receptor} \rightarrow \text{periph. axon} \rightarrow \text{dorsal-root ganglion} \rightarrow \rightarrow \text{ascending CNS pathways} $$
Pain is not an electrical signal stored inside an injured shoulder. Nociceptors detect potentially damaging mechanical, thermal, or chemical conditions. Their axons carry signals into the CNS, where spinal and brain networks combine that input with attention, prior experience, descending inhibition, sensitization, and the current state of the body.
TENS inserts additional structured activity into this pathway.
2. why axons are the target
A neuron has a cell body, dendrites, and an axon. The axon is the long cable used to move action potentials over distance. A peripheral nerve is not one wire; it is a bundle of many axons with connective tissue, blood vessels, and different sensory and motor functions.
Axons matter to TENS because they are electrically excitable. When an external electric field changes the voltage across an axonal membrane enough, voltage-gated ion channels open and an action potential begins.
A rough threshold model is:
$$ \text{fire} = \mathbb{1} \left[ V_{\mathrm{membrane}} \geq V_{\mathrm{threshold}} \right] $$
This is not a complete Hodgkin-Huxley model. It only shows the key nonlinearity: below threshold the pulse may produce no propagated response; above threshold an action potential can travel along the axon.
Myelinated axons conduct through saltatory conduction. The myelin electrically insulates most of the axon, while action potentials are regenerated at nodes of Ranvier. Larger, myelinated fibers generally conduct faster and can have lower electrical recruitment thresholds than smaller nociceptive fibers.
That gives conventional TENS part of its operating strategy: recruit large-diameter sensory afferents strongly enough to influence spinal processing without pushing the stimulation into painful cutaneous or unwanted motor recruitment.
3. the sensory fibers are not interchangeable
A simplified fiber map is:
| Fiber group | Typical structure | Main relevant function | Approximate sensation |
|---|---|---|---|
| A-beta | large, myelinated | touch, pressure, vibration | tingling, tapping, buzzing |
| A-delta | smaller, thinly myelinated | fast nociception, cold | sharp or pricking sensation |
| C fibers | small, unmyelinated | slow nociception, warmth, itch | burning or aching sensation |
| Motor axons | large, myelinated | skeletal-muscle activation | twitch or contraction |
This table is a simplification. A surface electrode does not select one fiber class perfectly. Recruitment depends on axon diameter, depth, orientation, distance from the electrode, pulse width, and the local field.
The point is that “I can feel electricity” does not uniquely identify what the unit recruited. A comfortable buzzing sensation, a sharp sting, and a visible trapezius twitch are different outputs from the same general hardware.
TENS and NMES also get mixed together. TENS is generally used for sensory neuromodulation and pain relief. NMES recruits motor axons to produce contractions. Combination units can contain both modes, which makes the real waveform more important than the type itself.
4. how a surface pulse reaches an axon
The current has to cross the electrode-gel interface, stratum corneum, deeper skin, fat, fascia, and other tissue before it reaches a target nerve.
A basic electrical model is:
$$ I = \frac{V} {Z_{\mathrm{skin}}} $$
$I$ is delivered current, $V$ is applied voltage, and $Z_{\mathrm{skin}}$ is effective impedance. Impedance changes with hydration, electrode adhesion, hair, movement, pad age, and frequency. That is why the same setting can feel different between sessions.
The local current density is:
$$ J = \frac{I} {A_{\mathrm{contact}}} $$
If a pad peels up, the effective contact area falls and current can concentrate near the remaining edge. The display may still say level 8, while the skin exposure has changed.
Charge per phase is:
$$ Q_{\mathrm{phase}} = Iw $$
$w$ is pulse width. At a fixed current, a longer pulse delivers more charge and gives the membrane longer to depolarize. This is why mA alone is not a dose.
5. strength-duration explains why the controls interact
Axonal excitation follows a strength-duration relationship. Short pulses generally require higher current to reach threshold; longer pulses can reach threshold at lower current.
A classic approximation is:
$$ I_{\mathrm{threshold}} = I_{\mathrm{rheobase}} \left( 1+ \frac{t_{\mathrm{chronaxie}}} {w} \right) $$
$I_{\mathrm{rheobase}}$ is the minimum current approached at long pulse widths. $t_{\mathrm{chronaxie}}$ describes the time scale of excitability, and $w$ is pulse width. The equation is useful for thinking about parameter tradeoffs. It cannot predict a safe home setting because the actual threshold also depends on anatomy, electrodes, waveform, and the specific axons being recruited.
A 2025 computational study used a detailed forearm model and an axon model to examine TENS pulse widths from 30 to 495 microseconds. Its modeled median-nerve threshold decreased as pulse width increased. At a fixed current, the predicted volume of activated tissue increased w/ pulse width.
Those values came from one simulated anatomy and placement. They are not a dosing chart. The useful result is the shape of the relationship.
6. what happens in the spinal cord
Nociceptive afferents enter the dorsal horn of the spinal cord and synapse onto spinal neurons that participate in ascending pain pathways, reflexes, and local circuits.
The gate-control explanation of TENS is basically that strong non-noxious afferent input can recruit inhibitory spinal interneurons and reduce transmission from nociceptive inputs to projection neurons.
A rough balance is:
$$ N_{\mathrm{out}} = N_{\mathrm{nociceptive}} – G_{\mathrm{segmental}} – D_{\mathrm{descending}} $$
$N_{\mathrm{nociceptive}}$ is incoming nociceptive drive. $G_{\mathrm{segmental}}$ is local inhibitory influence associated partly w/ competing sensory input. $D_{\mathrm{descending}}$ represents inhibition from brainstem and other CNS networks. The output is not a directly measurable pain value; it is a model of how several inputs could change onward transmission.
This is why rubbing an injured area and using conventional TENS are conceptually related. Both add non-noxious somatosensory input. TENS is more controllable because the waveform can be repeated, moved, and titrated.
Low-frequency, higher-intensity stimulation may also engage motor afferents and descending opioid-related systems. Experimental studies link TENS with endogenous opioids, serotonin, acetylcholine, noradrenaline, and GABA. The human clinical literature does not give us a clean table where one exact frequency always produces one neurotransmitter response.
7. the main TENS modes are different neural strategies
conventional TENS:
higher frequency, lower pulse width, strong non-painful paresthesia
goal: mainly sensory-afferent recruitment and segmental inhibition
acupuncture-like TENS:
lower frequency, higher intensity, often visible muscle twitch
goal: motor-afferent input and broader descending modulation
intense TENS:
high frequency and high tolerable intensity for short use
goal: counter-irritation and stronger afferent blockade/modulation
The labels describe physiological intentions better than consumer names like “cupping,” “massage,” or “shoulder.” A device can call a program “deep tissue” without measuring depth or knowing where the target nerve sits.
From what I understand, the most defensible conventional TENS instruction is still to create a strong but comfortable, non-painful sensation near the painful area. It should be an adjustable sensation, not a contest to tolerate the highest number.
8. therapeutic dose vs. harmful dose
There is no universal boundary where 10 mA is therapeutic and 15 mA is harmful. The operating window is person-, site-, waveform-, electrode-, and session-specific.
One way to normalize it is:
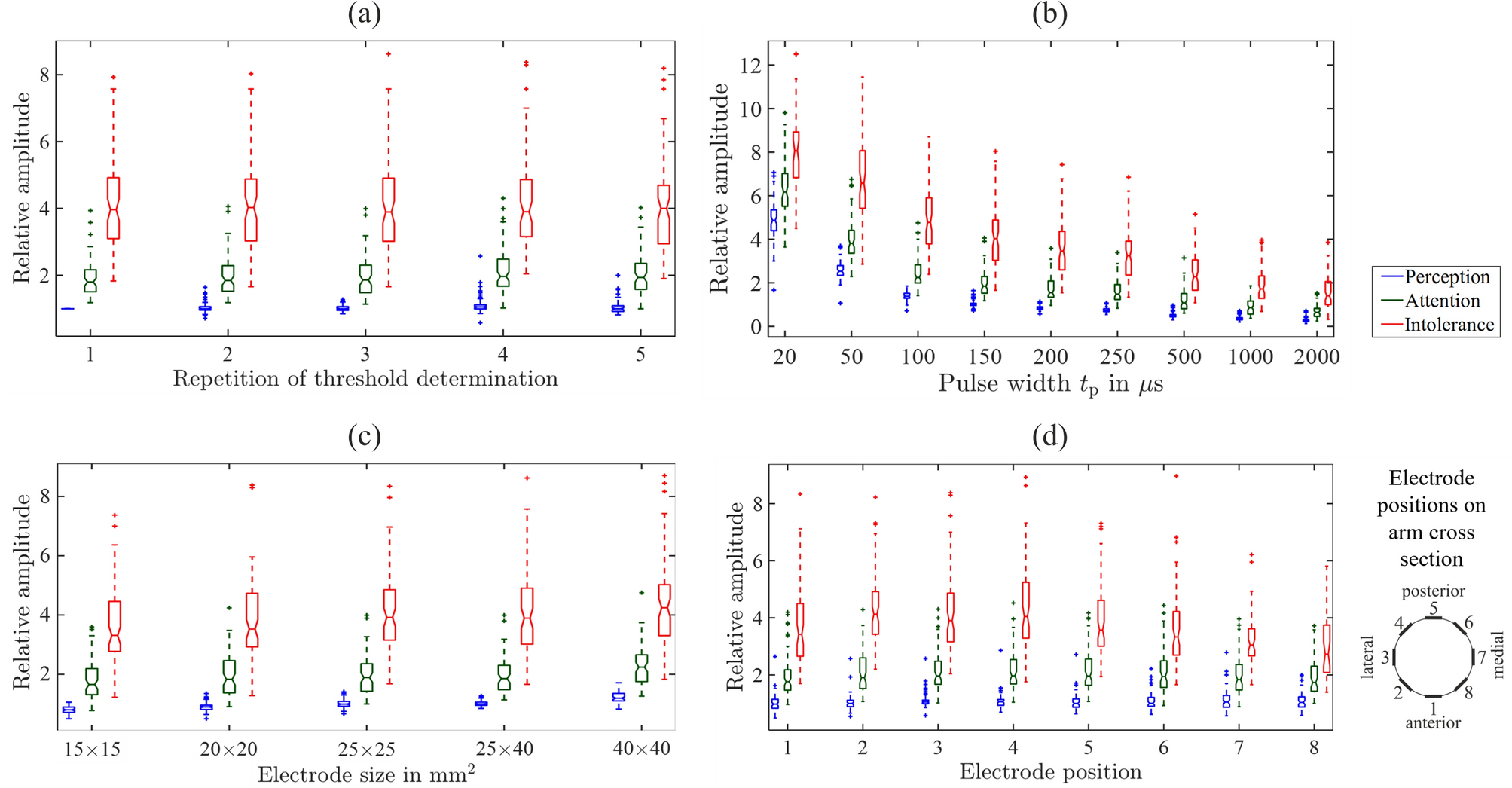
$$ D = \frac{ I_{\mathrm{used}} – I_{\mathrm{perception}} }{ I_{\mathrm{intolerance}} – I_{\mathrm{perception}} } $$
$I_{\mathrm{perception}}$ is where the current is first felt. $I_{\mathrm{intolerance}}$ is where the current becomes intolerable under that setup. $D$ places the chosen amplitude inside the individual sensory window. It cannot prove analgesia or safety, but it is more meaningful than saying “level 7.”
In a study of 81 healthy volunteers receiving 150-microsecond biphasic electrocutaneous pulses on the upper arm, median perception, attention, and intolerance thresholds were 3.5, 6.9, and 13.8 mA. The distributions varied across people, and thresholds fell as pulse width increased. These were experimental thresholds, not therapeutic limits.
Potential harm depends on more than discomfort:
high local current density
partially detached or dried electrodes
long exposure without skin checks
damaged or inflamed skin
reduced protective sensation
unsafe placement
unintended muscle contraction
interaction with an implanted electronic device
Pads should not be placed across the chest, on the front or side of the neck, over damaged skin, or where the device labeling excludes use. Implanted electronic devices, impaired sensation, pregnancy, epilepsy, and other cautions require clinician- and device-specific review.
9. why different people feel the same setting differently
The device sees an electrical load. It does not see nerve depth, subcutaneous thickness, neuropathy, sensitization, skin hydration, anxiety, or whether the pad is centered over a superficial nerve branch.
Two people can receive the same programmed pulse and experience different fields at the nerve. The same person can also change across sites and days.
Peripheral neuropathy may raise, lower, or distort sensory thresholds. Central sensitization may change the relationship between input and perceived discomfort. Habituation can make a constant stimulus feel weaker during a session, which is why some protocols retitrate intensity while maintaining comfort.
10. what the evidence supports
The 2022 metaTENS study included 381 randomized trials and 24,532 participants. Across 91 placebo-controlled trials, pain intensity during or immediately after TENS favored TENS, with moderate-certainty evidence. The review focused on strong, non-painful stimulation at or near the painful area.
The evidence was much weaker for duration of benefit, condition-specific effects, and adverse-event estimates. Many trials were small, protocols varied, and treatment parameters were incompletely reported.
This helps reconcile personal benefit w/ cautious guidelines. TENS can reduce pain during or immediately after use without repairing the pathology or becoming a recommended routine treatment for every chronic pain diagnosis. NICE recommends against routine TENS for chronic primary pain and low-back pain, and the WHO made a conditional recommendation against it for chronic primary low-back pain.
My own use tells me the output can feel meaningful. It doesn’t tell me whether the original injury healed faster or which tissue produced the pain in the first place though
11. other use cases are different targeting problems
Transcutaneous stimulation can target other peripheral pathways.
Transcutaneous tibial nerve stimulation places electrodes near the ankle to influence sacral circuits involved in bladder control. It has been studied for overactive bladder. The target, outcome, and treatment schedule are different from local TENS over an aching back.
Electrocutaneous stimulation can also serve as an information channel. Research systems use patterned pulses for prosthetic feedback, navigation, warnings, and teleoperation. The objective becomes a distinguishable sensation without pain or unintended movement.
Wearable garments could improve placement repeatability by integrating textile electrodes. Their engineering problem is maintaining pressure, hydration, impedance, washability, and electrical isolation during movement.
TENS could also be synchronized with rehabilitation. A device could detect the movement phase that usually produces pain, deliver a bounded pulse sequence, and test whether range of motion changes.
12. moving from open-loop to closed-loop
Most TENS units are open-loop:
$$ \text{user setting} \rightarrow \text{fixed stimulation} $$
A closed-loop unit would observe the state and adapt within validated limits:
$$ \text{sensors} \rightarrow \text{state estimate} \rightarrow \text{bounded stimulation} \rightarrow \text{response} \rightarrow \text{update} $$
Useful sensors include electrode impedance, surface EMG, motion, pad contact, and perhaps heart-rate or electrodermal features. The main missing input is still the person’s report and function. A perfect EMG signal does not tell the device whether neck rotation became less painful.
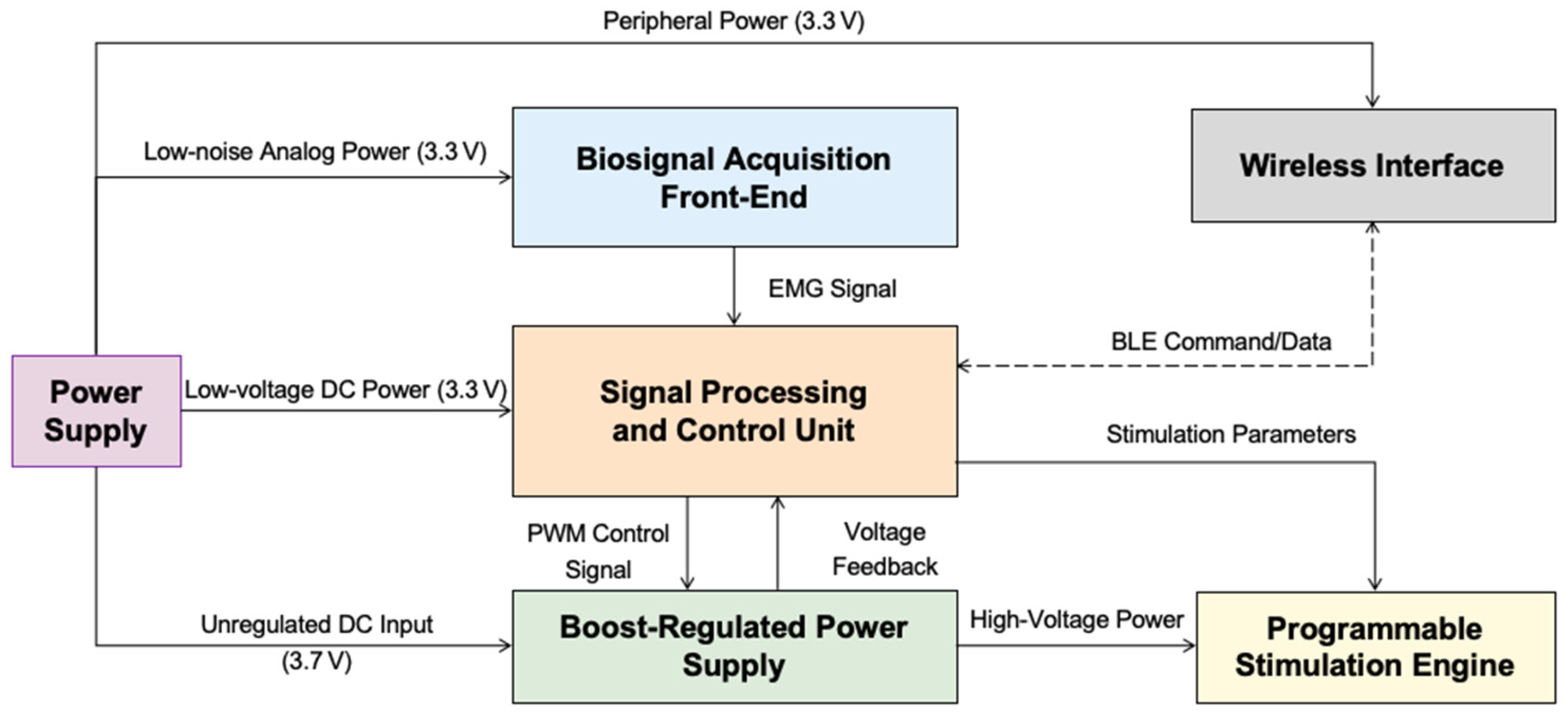
A 2025 paper described a six-channel wearable prototype using surface EMG to trigger TENS with less than 10 milliseconds of bench-tested loop latency. Its human analgesia protocol was still pending approval. It demonstrated an interesting hardware architecture, not established clinical benefit.
13. where neural networks fit
I would not begin with a neural network claiming to detect pain from heart rate, facial expression, or one wearable signal. Pain labels are subjective and confounded by movement, stress, medication, and expectation.
The first model could be a contextual bandit or Bayesian optimizer learning within one user:
$$ a_t^* = \arg\max_{a\in\mathcal{S}} \mathbb{E} \left[ R_t \mid x_t,a \right] $$
$x_t$ contains impedance, pad map, movement, baseline pain, prior response, skin symptoms, and waveform history. $a$ is a candidate stimulation action from a prevalidated safe set $\mathcal{S}$. $R_t$ is a functional outcome such as pain during shoulder abduction plus duration of relief. The model ranks safe actions; it does not invent new electrical outputs.
With a larger longitudinal dataset, a temporal CNN or transformer could process multichannel sequences from EMG, accelerometry, impedance, and device output. It could predict contact loss, movement-evoked symptoms, or response decay.
The deterministic safety controller should remain separate from the neural network. A model error should not be able to exceed charge, current-density, session-duration, placement, or temperature limits.
14. what data should actually be collected
patient and pathology context
pain location and duration
suspected nociceptive, neuropathic, or mixed mechanism
injury or diagnosis
medications
sensory impairment
implanted-device status
prior response to TENS
electrical delivery
current amplitude
pulse width
frequency
waveform and polarity
session duration
electrode size and spacing
measured impedance
amplitude changes during use
placement and operation
pad coordinates on a body map
target nerve, dermatome, or painful region
electrode age and contact quality
movement state
device and firmware version
timestamps
outcomes
pain before, during, and after stimulation
task-specific function
time until pain returns
sleep interruption
rescue medication
skin irritation
unintended contraction
reason for stopping
15. the legal boundary moves when the device learns
In the U.S., a TENS device for pain relief is generally Class II under 21 CFR 882.5890. Many products use the FDA 510k pathway and compare themselves with their legally marketed predicates. Clearance supports the cleared intended use. It does not show that every preset is superior or that the device repairs an injury.
If software changes stimulation based on patient data for pain treatment, the software is part of the medical-device function. New indications, materially different waveforms, or a learning control policy can change the premarket analysis.
FDA guidance allows an AI-enabled device submission to include a Predetermined Change Control Plan. The plan describes bounded future modifications, the method for developing and validating them, and the assessment of their effect. It is not permission for a deployed model to rewrite its control policy without review.
Since February 2, 2026, FDA’s Quality Management System Regulation incorporates ISO 13485:2016 into the U.S. framework. Model monitoring, supplier controls, complaints, firmware changes, electrode failures, and corrective actions belong in that quality system.
HIPAA also does not automatically cover a consumer TENS app. It depends on whether the company is a covered entity or business associate. A direct-to-consumer product may instead fall under the FTC Act and the FTC Health Breach Notification Rule. Pad-location photos, pain diaries, activity traces, and device identifiers are sensitive health data even when HIPAA is not the applicable law.
16. graphs i found cool
median-nerve strength-duration curve
modeled threshold current falls as pulse width increases, showing why pulse width and mA cannot be interpreted separately.

predicted activation volume vs. pulse width
in one forearm model, predicted volume of activated tissue increased w/ pulse width at a fixed current. This is anatomy- and model-specific.

perception, attention, and intolerance thresholds
experimental thresholds across pulse widths show that the felt operating window changes w/ waveform and varies across people.
EMG-driven closed-loop TENS architecture
prototype architecture combining biosignal acquisition, real-time control, programmable stimulation, and a regulated power stage.
17. the thesis
The simplest useful statement is:
$$ \text{TENS value} = \frac{ \text{functional analgesia from recruited neural pathways} }{ \text{discomfort} + \text{skin risk} + \text{treatment burden} } $$
The numerator depends on which peripheral axons are recruited, how that activity changes spinal and descending CNS processing, and whether the change improves a defined task. The denominator captures the limits that stop “more current” from being the objective.
TLDR. My personal learning: TENS matters because pain signals and competing sensory signals travel through axons connecting the PNS to the spinal cord and brain. Surface pulses can recruit peripheral sensory fibers, alter inhibitory processing in the dorsal horn, and influence descending CNS pathways, which can reduce perceived pain during or shortly after stimulation. The main technical limitation is that current devices label a few open-loop waveforms as body-part presets while ignoring the person-specific electrical path, axon thresholds, electrode contact, functional response, and changing sensory window. A better TENS system would measure the actual electrical dose and impedance, preserve electrode location, test movement-level outcomes, personalize only inside a validated action set, and keep hard safety limits outside the neural network.
Comments are closed for this post.